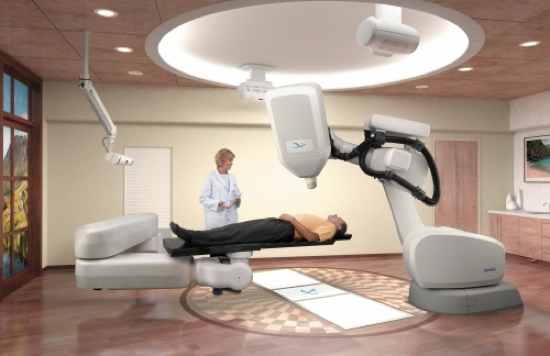
In December 1983-February 1984, in Ciudad Juarez, Mexico, and the United States, occurred one of the first widely reported cases of radiation exposure from the inadvertent destruction of orphaned sources through the scrap metal recycling process. On December 6, 1983, a used metal teletherapy unit (pictured) containing a source container with about 6,000, one-millimeter pellets, each with radioactive cobalt 60, was deliberately opened in a scrap yard in Ciudad Juarez, Mexico. The pellets were scattered throughout the scrap yard, and a magnetic loader further dispersed the radioactive pellets, when the scrap metal was converted to steel products on December 10, 1983. Contaminated products included steel rebar and table pedestals, manufactured from the contaminated steel and shipped to the US. The contamination went undetected until January 16, 1984, when a truck carrying the contaminated rebar took a wrong turn at the Los Alamos, New Mexico, scientific laboratory and set off an automatic radiation sensor. Later that same day, five more trucks carrying contaminated steel were stopped at the Mexican border, near El Paso, Texas. Over the following weeks, about 900 tons of contaminated steel were identified and recovered in the US. Some of the contaminated table parts had already been made into finished tables and had to be retrieved from restaurants. In February, 1984, Mexican officials determined that ten individuals had been exposed to high levels of radiation. One of these subsequently died from their injuries. An aerial survey of the Ciudad Juarez area in March of that year, located 21 contaminated zones including a pickup truck with children playing on it. In Sinola, Mexico, authorities had to destroy 109 homes that had been built with the contaminated rebar.
Another orphaned source event occurred in March, 1984, in Morocco. This time the orphaned source was an iridium-132 source. Many individuals received significant overdoses of radiation that required medical attention, and eight people died. The source was used to radiograph welds – a non destructive analysis where ionizing radiation is used to look for defects in the metal that cannot be seen any other way. The source became separated from the shielded container used to store it, and the source itself had no markings indicating it was radioactive. Somehow, a worker found the source and took it home, where it stayed for some weeks, exposing the family to radiation.
On September 13, 1987, at Goiania, Brazil, a radioactive source was removed from an abandoned hospital in the city. Over time, the radioactive source was handled by multiple people, and led to the exposure to high levels of radiation of at least 245 people. Twenty of those showed sign of radiation exposure and needed hospital treatment. At least four people died. This time it was a cesium-137 source, which had been left behind when a private radiotherapy institute moved to a new location. Left unsecured for two years, it was eventually located by scrap hunters scavenging for metal. Not knowing what they had, the scavengers took the unit home, tried to open it and in the process, damaged the cesium-137 source. This led to the contamination of hundreds of people as well as the environment, which resulted in a six-month radiation clean up. More than 100,000 people ended up being monitored for radiation as a result.
Radioactive sources have many uses, and not just for medical purposes. One such use is sterilization of medical instruments, and even food products. A high energy cobalt-60 radioactive source was being used at just such a plant in Soreq, Israel, in June, 1990, when the source used in the irradiation process became stuck in its rack. Two conflicting warning signs were provided to the operator of the irradiation machine, which may have confused him. He bypassed the safety systems designed to prevent an operator from being exposed, and came up with procedures so that he could enter the irradiation room and free the blockage. As a result, the operator entered the room and was, himself, irradiated. He was exposed to high levels of radiation and died only a month later. Tragically, this was not the first, nor would it be the last incident involving a source which had become stuck in such a facility. In February, 1989, in San Salvador, El Salvador, a cobalt-60 source became stuck and again, workers bypassed safety systems and entered the irradiation room. This time, three men went into the room to free the stuck source. In the process, all three received high doses of radiation. The legs and feet of two of the men were so burned by the radiation that they had to be amputated. The third man died six months later. In October, 1991, in Nesvizh, Belarus, a cobalt-60 source became jammed in the product transport system and the operator entered the facility to clear the blockage, once again, bypassing several safety systems. The source became active for about one minute and the operator was exposed to high levels of radiation as a result. He was taken for special medical treatment in Minsk, Russia, but died 113 days later.
At a hospital clinic located in Zaragoza, Spain, between the dates of December 10 and December 20, 1990, at least 27 patients who were receiving radiotherapy for cancer were accidentally exposed to high levels of radiation, which resulted in the deaths of 11 patients, and severe injuries to the others. On December 7, 1990, maintenance was performed on the electron accelerator used to treat cancer patients at the clinic. The unit was started again the following day, December 10. The Spanish Nuclear Safety Board inspected the unit, and found the power of the electron accelerator was set too high, and it was taken out of service on December 20, 1990. But, by then, many patients had been exposed to higher than expected, and unsafe, levels of radiation. The affected patients immediately suffered skin burns and effects to internal organs and their bone marrow. The first patient died on February 16, 1991. The last fatality occurred on December 25, 1991. The 14 year old instrument had a breakdown in the electron beam accelerator control system. The service man who repaired the instrument incorrectly increased output power, so patients that should have received therapy at 7 million electron volts (MeV) were instead treated at 40 MeV. The hospital manager blamed the technician, and the Spanish Health Minister blamed GE, the manufacturer of the instrument. After a court hearing, the technician and GE were found to be at fault. The device was taken out of service and disposed of, in 1996.
In November, 1992, an 82 year old patient was undergoing brachytherapy radiotherapy treatment at the Indiana, Pennsylvania, Regional Cancer Center. While undergoing treatment, a 3.7 curie iridium-192 source dislodged from the equipment and was accidentally left inside the patient. The error went unnoticed because the staff did not conduct routine inventory checks of all radioactive sources. The patient died 93 hours later, at her nursing home, from exposure to radiation from the source. The catheter containing the source was removed from the woman and disposed of as normal medical waste. The waste disposal company discovered the radioactive source during routine checks for radioisotopes. The subsequent Nuclear Regulatory Commission (NRC) investigation found that 94 individuals at the center, the nursing home and the waste disposal company had been exposed to radiation.
In October, 1994, in Tommiku, Estonia, three brothers somehow managed to gain entrance into a facility used to store radioactive waste. They had no authorization to enter this facility. Inside they found a metal container and removed it from the facility. Inside the metal container was a radioactive source. They were able to open the container and expose themselves to the radiation from the source. The radiation exposure killed one of the three brothers, and led to the exposure of many others. At first the man’s death was not linked to radiation exposure. However, upon examining the radiation injuries of another family member, a physician realized they were all related to radioactivity. The physician alerted authorities who were able to contain the damage from being worse than it otherwise would have been.
In August, 1996, a radioactive cobalt-60 source was replaced in an Alcyon II radiotherapy instrument, at the San Juan de Dios Hospital, in San Juan, Costa Rica. An error was made in calculating the dose rate when the instrument was restarted. Before the error was caught in September, 1996, 115 patients who had been treated using the instrument had been exposed to significantly higher levels of radiation than expected. Later calculations would estimate the over exposure at 50-60% greater levels of radiation than intended. By July, 1997, nine months after the accident, 42 of those patients had died. All of the patients showed classic signs and symptoms of over exposure to radiation.
The device involved in this incident was a Gammatron-3 teletherapy unit, originally installed in a Bangkok, Thailand, hospital, in 1969. The tele therapy unit has a source holder and shield made from lead, and surrounded by stainless steel. It weighed about 280 pounds. In the center of the holder was the cobalt-60 source. The tele therapy unit had been taken out of service by the hospital many years previously, and had been in storage, along with several other pieces of radioactive machinery, in another location. Eventually, three of these units were moved to a garage and it was there that the one tele therapy unit was stolen for sale as scrap metal. On January 24, 2000, two men purchased the tele therapy unit as scrap metal, and drove it through Bangkok to their home. On February 1, 2000, these two men, along with a third man, tried to pry apart the unit but were unsuccessful. They then gave up and decided to take the unit to a scrap yard. Along with a fourth man, they drove the unit to the scrap yard, but first stopped at one man’s home. While there, one of the men sitting in the car draped his one leg over the unit. At the scrap yard, the men asked the scrap yard employee to use a torch to cut open the unit, which he did. A second employee of this scrap yard was positioned behind the employee who used the torch to cut thorough the stainless steel box and lead cylinder. A yellow, foul smelling smoke came from the unit and two pieces fell out onto the ground. The man with the torch picked them up. The man said his hands felt “itchy” while holding the pieces. The female owner of the scrap yard came out and ordered the men to take the unit back to their house, and continue working on it there. They put the, now cut open, tele therapy unit back into their car and drove back home. Though they began to feel sick and nauseous, they did manage to finally separate the stainless steel and lead assemblies, and returned with them to the scrap yard the next day. In total, the four men who had obtained the tele therapy unit, and six people at the scrap yard, including the man who cut it open with a torch, the man working beside him, the female owner, her husband and two others were exposed to high levels of radiation. By mid February all had developed signs of radiation sickness, and had been admitted to hospitals. The treating physician noticed the people were suffering from apparent radiation exposure, and contacted Thailand authorities who dispatched two health physicists to investigate. Using a radiation meter and driving through the area near the scrap yard, the eventually noticed higher than normal radiation levels and determined the location of the radioactive source. Unfortunately, the source was buried in amongst tons of other scrap metal. Authorities then spent many days carefully removing pieces of scrap metal until they were finally able to locate the actual source and safely remove it. They also found and seized control of the other tele therapy units sitting unprotected in the garage. Of the four men who originally handled the unit, one had to have body parts amputated and the other, who had his leg over the unit, had severe radiation burns to the leg. But all survived. Of the six individuals exposed at the scrap yard, the man who cut open the unit and the man who worked next to him both died. In addition, the husband of the scrap yard owner died of his injuries.
In April, 2010, the locality of Mayapuri, India, was affected by a serious radiological accident when a Gammacell 220 research irradiator, owned by Delhi University, was sold at auction to a scrap metal dealer in Mayapuri, on February 26, 2010. The source, unused since 1985, had been removed from the university and sold off as scrap, thus becoming what is known as an “orphan source”. Strict rules and regulations require owners of radioactive sources to always know where the source is located, and never lose control of the source. This did not happen in the Mayapuri event, and orphan sources, as we have seen, are potentially deadly. The cobalt-60 radioactive source was cut into several pieces by the scrap metal workers, one of whom took a piece and put it in his wallet. Two more pieces were taken to a nearby shop, and the remaining eight pieces were left in the scrap yard. All of the pieces of the source were eventually recovered in mid-April, and sent to a nuclear power station. As a result of cutting the source into pieces, eight people were hospitalized due to radiation exposure, and one died.
I included the Yanango incident even though, as far as I have been able to determine, the exposed man has not yet died. However, the extent of his injuries are so severe there is little doubt that if he is still alive, he will eventually die as a result. If you would like to read the full investigation report by the IAEA go here. Be warned, the photographs of the man’s injuries are extremely graphic. In February, 1999, a hydroelectric plant was under construction in Yanango, Peru, several hundred miles east of Lima, Peru. On the morning of February 20, 1999, a welder and his assistant began to conduct repairs on a pipe. Soon a radiographer arrived to take radiographs of the welds and the pipe in order to ensure the pipe was safe to conduct hydrostatic testing. But the welding was not yet finished, so the radiographer left – leaving the radiograph camera, locked but unsupervised, at the construction site. The camera is essentially a metal box with a “source pigtail” which is a pencil-length long braided metal connector that looks nothing at all like something anyone would think contains radioactivity. In fact, the source pigtail contained an iridium-192 radioactive source. The pigtail is inserted into the camera with one end protruding slightly. That end of the source pigtail is then connected to drive cable. The welders resumed their work. Soon the radiographer went to use the camera, but it failed. Somehow, the pigtail fell out of the camera (there were locks in place that should have prevented this from happening, but still, the pigtail fell out). The radiographer left the construction site and, not knowing the danger, one of the welders picked up the pigtail with his right hand and put it in his back right pocket. The welder continued to work for another three hours, then boarded a bus with multiple other workers and went home. Before he left work he began to notice a pain in his right thigh. At home the man complained to his wife about the pain and took off his pants. The wife noticed a red spot on his thigh and the man went to a local doctor who told him he had a bug bite. While he was gone the wife breastfed their infant child and two other young children played in the area where the pants, and the pigtail in the pocket, were laying on the floor. Once back home the man remembered the pigtail he had picked up and realized it was still in his back pocket of his pants. He took the pigtail out of his pocket with his right hand and carried it outside to the outhouse. Later, the plant operator came to the man’s house asking if he had seen the missing source. The man went to the outhouse, picked up the pigtail with his right hand, and carried it back to the house to show the operator. Upon seeing the pigtail in his hand, the operator told the man to toss it into the street. Later the pigtail was safely retrieved and the street and house decontaminated. But it was too late for the welder. After aggressive treatment in Peru, the man was flown to France for some of the most cutting edge treatment available. Still, by February 2000, one year after the incident, the man had lost his entire right leg and buttock and had significant infection in other areas of his body, including his left leg and right hand. In addition, from sitting on his pants, his wife had a small radioactive burn on her buttock.